
Sleep & Physical Therapy — The Science of Restorative Recovery
Highlights
• Sleep is now a measurable treatment outcome in physical therapy, not just a symptom.
• Exercise therapy, when tailored for circadian rhythm and recovery, improves sleep quality in chronic pain and fatigue cases.
• Evidence-based physical therapy interventions help regulate the autonomic nervous system, promoting deeper and more restorative sleep cycles.
• Integrating Cognitive Behavioral Therapy for Insomnia (CBT-I) with physical therapy achieves superior results versus either alone.
• Digital physical therapy and tele-rehab platforms are expanding access to personalized sleep-rehab programs worldwide.
• Evidence-based patient section and clinicians’ technical section.

Why Sleep is the Missing Link in Recovery
Sleep is not a luxury; it’s a biological necessity for healing. During deep sleep, your body releases growth hormone, repairs tissues, and consolidates new motor skills learned in physical therapy. When sleep is poor, pain feels sharper, energy drops, and recovery slows. In fact, up to 80% of people with chronic pain also experience disrupted sleep, creating a self-reinforcing loop of fatigue and discomfort.
At Al Amal Physical Therapy Center, we treat sleep as a core modifiable factor, just like exercise, posture, and nutrition to optimize rehabilitation outcomes.
How Physical Therapy Improves Sleep

Recent high-quality research shows that structured physical activity as well as behavioral interventions can significantly improve sleep duration, quality, and efficiency.
- Aerobic Exercise: Moderate-intensity activity (brisk walking, cycling, or treadmill training) 3× per week improves sleep onset and total sleep time.
- Resistance Training: Two weekly sessions reduce insomnia severity and improve deep sleep cycles.
- Mind–Body Modalities: Yoga, tai chi, and Pilates enhance relaxation, lower stress hormones, and regulate circadian rhythms.
- Physical therapy-led Cognitive Behavioral Therapy for Insomnia (CBT-I): Physical therapists with training in cognitive behavioral strategies can incorporate sleep scheduling, stimulus control, and sleep hygiene into routine rehabilitation sessions. This emerging approach is supported by evidence from randomized controlled studies.
Takeaway: Exercise and sleep support each other. The right activity dose, delivered by trained physical therapists, can improve both your rehabilitation outcomes and your sleep quality.
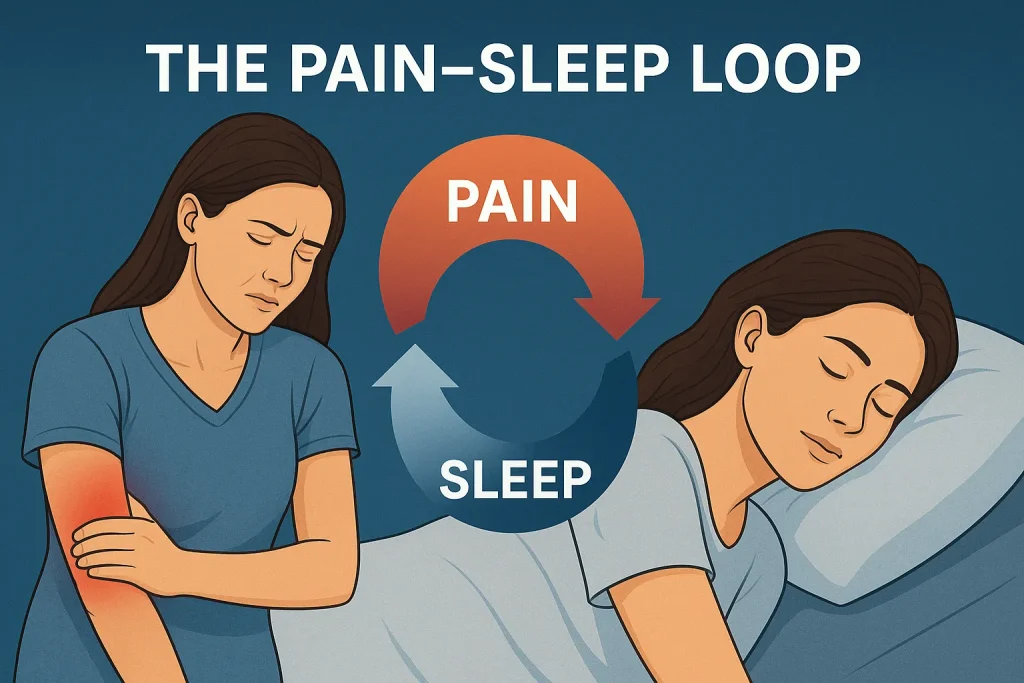
The Pain–Sleep Loop: Why physical therapists Must Act
Chronic pain disrupts sleep. In turn, lack of sleep amplifies pain perception by sensitizing the nervous system. This bidirectional link, known as the pain–sleep loop, is now recognized as a major obstacle to recovery.
Physical therapists are uniquely positioned to break this loop through:
- Education: Helping patients understand how movement, pacing, and relaxation influence sleep regulation.
- Exercise prescription: Graded aerobic and resistance training to reduce hyperarousal and improve metabolic recovery.
- Behavioral interventions: Integrating sleep hygiene education, relaxation breathing, and mindfulness training into treatment sessions.
Moreover, when these two approaches are combined, patients tend to experience fewer pain flares, faster healing, and greater mood stability. Thus, overall physical and psychological recovery is accelerated.
Our Clinic’s Evidence-Based Sleep Integration Protocol
Screening & Assessment

Every new patient completes a brief sleep screen:
- “Do you have trouble falling or staying asleep three or more nights per week?”
- “How would you rate your sleep quality in the past month (0–10)?”
If positive, standardized tools are administered to track progress.
Exercise Prescription for Sleep
- Frequency: 3–5 sessions/week.
- Duration: 30–45 minutes per session.
- Intensity: Moderate rate of perceived exertion (RPE) 11–14.
- Type: Combination of aerobic, resistance, and relaxation exercises.
Meanwhile, individualized exercise timing plays a crucial role. Evening stretching, breathing drills, and mind–body activities are prioritized for patients struggling with sleep onset, whereas early-day exercise proves most effective for those with morning fatigue.
Behavioral Sleep Coaching
During physical therapy sessions, clinicians often also deliver brief yet focused guidance on:
- Consistent sleep–wake timing.
- Reducing screen exposure 60–90 minutes before bed.
- Managing caffeine and alcohol.
- Relaxation techniques such as diaphragmatic breathing or guided imagery.
These are core elements of CBT-I, now being adapted for physical therapy delivery.
Relaxation and Autonomic Regulation

In-session techniques like Heart rate variability (HRV) biofeedback, slow breathing, and progressive muscle relaxation are used to reduce physiological arousal. Studies show these practices lower cortisol and improve sleep onset latency.
Referral Pathway
Patients with suspected sleep apnea, restless legs syndrome, or excessive daytime sleepiness are referred to sleep medicine specialists for polysomnography and targeted care.
Patient Section — 5 Quick Sleep Tips Backed by Science
- Stick to a schedule: Go to bed and wake up at the same time every day.
- Exercise regularly: Even short daily movement sessions improve sleep quality.
- Create a wind-down routine: Dim lights, stretch gently, and do slow breathing.
- Keep your room cool, quiet, and dark.
- Limit caffeine & alcohol: avoid after mid-afternoon; both fragment sleep.
If sleep issues persist despite these steps, discuss with your physical therapist you may benefit from specialized sleep-focused rehabilitation.
FAQ
Technical Section (for clinicians & researchers)
Implementation Roadmap for Clinics
First Phase: Staff training (two 8-hour workshops) on sleep screening, exercise dosing, and CBT-I basics.
Second Phase: Launch a 12-week pilot with weekly clinician huddles and patient feedback loops.
Third Phase: Publish outcomes and open datasets to attract research partners.
Clinics that adopt this model can lead national-level collaborations on pain and sleep rehabilitation.
Patient action (easy, 5 prescribed steps)
- Regular sleep window: pick a bedtime and wake time the patient can keep every day (±30 minutes).
- Move daily: aim for 30 minutes of moderate activity most days (walking, cycling, or a strength circuit). Exercise reliably improves sleep when done regularly. Avoid very intense exercise within 60–90 minutes of bedtime if it keeps the patient wired.
- Wind-down routine (30 minutes): dim lights, stop screens, do gentle breathing or stretching, and keep the bedroom cool and dark.
- Limit caffeine & alcohol: advise on avoiding after mid-afternoon; both fragment sleep.
- Use movement as medicine: short, targeted prescribed exercises (strength or low-impact aerobic) help sleep and recovery.
Clinic program
- Screening at intake: short sleep questions plus validated short scales (Insomnia Severity Index or Pittsburgh Sleep Quality Index when needed).
- Exercise prescription: dose-specific activities (aerobic and resistance/mind-body options) tailored to pain and fitness.
- Behavioral coaching: sleep hygiene, stimulus control basics, and sleep scheduling integrated into rehab visits.
- Relaxation & autonomic tools: guided breathing, brief HRV-aware exercises and progressive muscle relaxation in-session.
- Escalation pathway: refer for suspected sleep apnea, severe daytime sleepiness, or medication review.
Measured results
- Insomnia Severity Index (ISI)
- Pittsburgh Sleep Quality Index (PSQI)
- PROMIS Pain Interference
- Functional scales (LEFS, NDI)
- Actigraphy metrics (total sleep time, sleep efficiency)
Tracking these metrics allows the clinic to measure real-world impact and attract research or industry collaborations.
12-week sample program
- Weeks 1–4 (Foundations): moderate aerobic 30 min ×3/wk; 2 sessions resistance (20–30 min); evening wind-down 20 min; brief sleep coaching during each visit.
- Weeks 5–8 (Progress): increase aerobic to 40 min when tolerated or add mind-body class (yoga/tai-chi 2×/wk); start sleep consolidation (consistent sleep window).
- Weeks 9–12 (Maintenance): maintain exercise dose; add booster sessions for CBT-I skills (sleep restriction/stimulus control) if insomnia persists.
When to refer to sleep medicine (red flags)

- Loud snoring with witnessed apneas or choking/gasping during sleep.
- Excessive daytime sleepiness affecting safety (driving, work).
- Restless legs with disruptive periodic limb movements.
- Rapid weight gain with new snoring.
GET IN TOUCH
Ready to Start Your Journey to Recovery?
References
Bothelius, K., Jernelöv, S., Kaldo, V., Lu, C., Stråle, M., & Jansson-Fröjmark, M. (2024). Internet-based cognitive behavioural therapy for insomnia comorbid with chronic benign pain – A randomized controlled trial. Internet Interventions, 38, 100781. https://doi.org/10.1016/j.invent.2024.100781
Bu Z, Liu F, Shahjalal M, et alEffects of various exercise interventions in insomnia patients: a systematic review and network meta-analysisBMJ Evidence-Based Medicine Published Online First: 15 July 2025. doi: 10.1136/bmjebm-2024-113512
Korkutata, A., Korkutata, M., & Lazarus, M. (2025). The impact of exercise on sleep and sleep disorders. Deleted Journal, 2(1). https://doi.org/10.1038/s44323-024-00018-w
Malfliet A, De Baets L, Bilterys T, et al. Cognitive Behavioral Therapy for Insomnia in Pain Management for Nonspecific Chronic Spinal Pain: A Randomized Clinical Trial. JAMA Netw Open. 2024;7(8):e2425856. doi:10.1001/jamanetworkopen.2024.25856
Qian, J., Sun, S., Wang, M., Sun, Y., Sun, X., Jevitt, C., & Yu, X. (2025, October 22). The effect of exercise intervention on improving sleep in Menopausal women: A systematic review and meta-analysis. Frontiers. https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2023.1092294/full
Runge, N., Ahmed, I., Saueressig, T., Perea, J., Labie, C., Mairesse, O., Nijs, J., Malfliet, A., Verschueren, S., Van Assche, D., de Vlam, K., Van Waeyenberg, T., Van Haute, J., & De Baets, L. (2024). The bidirectional relationship between sleep problems and chronic musculoskeletal pain: a systematic review with meta-analysis. Pain, 165(11), 2455–2467. https://doi.org/10.1097/j.pain.0000000000003279
FAQs
Yes. Structured exercise and sleep coaching delivered during physical therapy improve sleep duration, quality, and reduce insomnia symptoms.
Moderate aerobic activity 3×/week, resistance training 2×/week, and yoga or tai chi for relaxation are all proven effective.
Better sleep often helps reduce pain severity and interference, boosts energy, and enhances rehab adherence. However, some situations call for a combined approach, including pain management, CBT-I, and a referral to a sleep medicine specialist.
Your physical therapist will refer you to a sleep specialist. Physical therapy complements medical treatment by improving breathing mechanics, posture, and aerobic fitness.




